
NORMAL LABOUR
Defintion- Labour is described as the process by which the fetus, placenta and memberane are expelled through the birth canal.
Normal labour occurs at term and is spontaneous in onset with the fetus presenting by the vertex. The process should be completed with acceptable time with in 24 hours vaginally. With no complications arise.
Definition
The physiological process by which the fetus, placenta, and membranes are expelled through the birth canal. The first stage of labour is from the onset of regular uterine contractions until full dilatation of the cervix.
- First stage of labour-The first stage of labour is the stage from the onset of true labour pains up to full dilatation of the cervix (10 cm).
Begins with-
- Regular painful uterine contractions
- Progressive cervical effacement and dilatation
Ends with-
- Full cervical dilatation (10 cm)
Phases of First Stage of Labour
1. Latent Phase
- Cervical dilatation: 0–4 cm
- Contractions are mild and irregular
2. Active Phase
- Cervical dilatation: 4–10 cm
- Contractions become strong, regular, and frequent
Note-WHO New Guideline(2018)-
- Cervical Dilatation in Latent Phase-0 cm to 5 cm
- Active Phase-Active labour begins at 5 cm cervical dilatation and continues to 10 cm.
Duration of First Stage of Labour
- In Primigravida (first pregnancy)-Average duration: 10–12 hours
- In Multigravida (woman with previous deliveries)-Average duration: 6–8 hours.
2. Second Stage of Labour
- Begins when the cervix is fully dilated
- Ends with the birth of the baby
- Mother pushes during contractions
Duration:-
- Primigravida About 1–2 hours
- Multigravida About 30 minutes–1 hour
3. Third Stage of Labour-The third stage of labour is the period from the birth of the baby until the expulsion of the placenta and membranes.
- Begins after the baby is born
- Ends with the delivery of the placenta (afterbirth)
Duration:-
- Normal duration Usually 5–15 minutes
- Maximum normal limit Up to 30 minutes
4. Fourth Stage of Labour
The fourth stage of labour is the period immediately following the delivery of the placenta during which the mother is kept under close observation for recovery and prevention of complications, especially postpartum hemorrhage.
It begins after the completion of the third stage and includes the early postpartum period.
- Duration: approximately 1–2 hours after delivery of the placenta.
Physiological changes in the first stage-
The onset of labour is a process, not an event. Cervical ripening takes place from 36 weeks’ gestation.
1. Cervical dilatation &Cervical effacemen-Cervical dilatation is the opening of the cervical os during labour due to uterine contractions and retraction. The cervix gradually opens to allow passage of the fetus through the birth canal.
Measurement
Dilatation is measured in centimeters (cm):
- Closed cervix – 0 cm
- Full dilatation – 10 cm
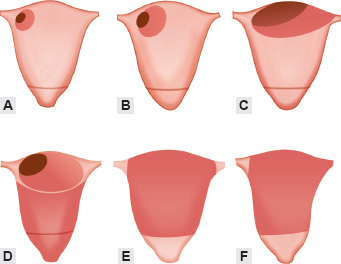
Cervical effacement is the thinning, shortening, and stretching of the cervix during labour. Before labour, the cervix is long and thick. With uterine contractions, the cervix gradually becomes soft, thin, and shorter to prepare for childbirth.
Measurement
Effacement is measured in percentage (%):
- 0% effacement – cervix is thick and uneffaced
- 50% effacement – cervix is half thinned
- 100% effacement – cervix is fully thinned out
Difference Between Cervical Effacement and Dilatation
| Cervical Effacement | Cervical Dilatation |
| Thinning and shortening of the cervix | Opening of the cervical os |
| Measured in percentage (%) | Measured in centimeters (cm) |
| Cervix becomes soft, thin, and shorter | Cervix becomes soft, thin, and shorter |
| Occurs mainly in early labour | Occurs progressively during labour |
| Helps prepare the cervix for delivery | Helps prepare the cervix for delivery |
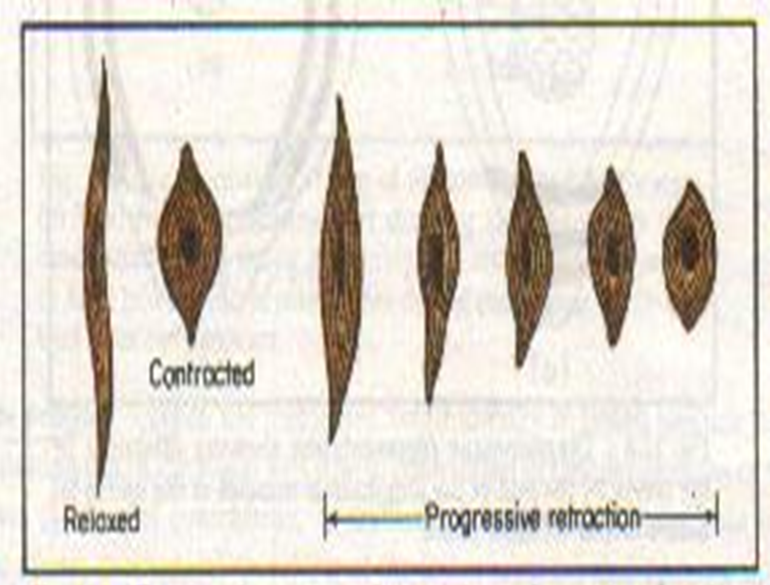
2. Contraction and retraction- Contraction refers to the temporary shortening and tightening of the uterine muscle fibers during labour. Uterine contractions occur rhythmically and intermittently, mainly in the upper uterine segment. During each contraction, the uterus becomes firm and hard, helping to push the fetus downward through the birth canal.
Retraction-Retraction is a unique property of the uterine muscle in which the muscle fibers do not return completely to their original length after each contraction. Instead, they remain slightly shortened. This permanent shortening mainly occurs in the upper uterine segment.
As retraction continues during labour:
- The upper uterine segment becomes thicker and shorter
- The lower uterine segment becomes thinner and stretched
- Progressive pull is exerted on the cervix, leading to cervical effacement and dilatation
Importance of Contraction and Retraction
Contraction and retraction together play a vital role in the mechanism of labour. They:
- Help in cervical dilatation and effacement
- Facilitate descent and expulsion of the fetus
- Aid in placental separation and expulsion
- Prevent postpartum hemorrhage by compressing uterine blood vessels after delivery
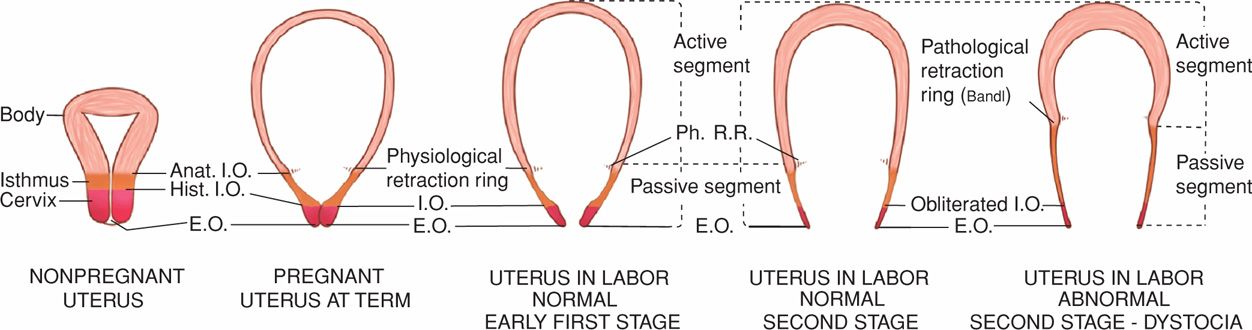
3. Retraction ring- A normal occurrence in all labours. Ridge formation occurs between the thick, retracted muscles of the upper segment and the thin, distended aspect of the lower segment. Only visible in obstructed labour, when a transverse ridge across the abdomen forms — known as Bandl’s ring — indicates imminent rupture of the uterus.
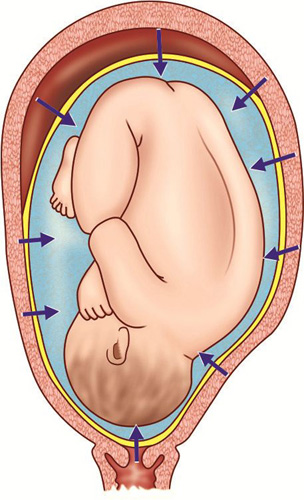
4. Fundal dominance-Fundal dominance is a characteristic of normal labour in which uterine contractions begin at the fundus (upper part of the uterus-uterine cornua) and spread downward toward the cervix. The contractions are strongest and longest in the upper uterine segment and gradually become weaker in the lower segment.
Importance
- Helps in cervical effacement and dilatation
- Pushes the fetus downward through the birth canal
- Assists in expulsion of the placenta
- Prevents postpartum hemorrhage by compressing blood vessels
Thus, fundal dominance ensures effective and coordinated uterine contractions during normal labour.
5. Upper active segment/lower passive segment- Shortening of the upper segment exerts pull on the passive lower segment. This initiates a reflex releasing oxytocin via the posterior pituitary, and assists with effacement and dilatation.
6. Polarity of the uterus- Polarity of the uterus is the harmonious coordination between the upper uterine segment and the lower uterine segment during labour. During each contraction, the upper segment contracts and retracts actively, while the lower segment and cervix relax and dilate.
Importance
- Promotes cervical effacement and dilatation
- Facilitates descent of the fetus
- Ensures normal progress of labour
- Helps in safe delivery of the baby
7. Resting tone- Resting tone is the minimum pressure maintained in the uterus between two uterine contractions during labour. Even during relaxation, the uterine muscles remain slightly tense and do not become completely relaxed.Normal resting tone is about 8–12 mmHg
8. Intensity of contractions- Contractions cause a rise in intrauterine pressure (amplitude), which can be recorded. Contractions rise rapidly to a peak, then slowly diminish (resting tone).
Uterine Pressure and Duration During Labour
| Stage of Labour | Pressure During Contraction | Duration of Contraction | Pressure During Relaxation |
| Early First Stage | 20–30 mmHg | 20–30 seconds | 8–12 mmHg |
| Active First Stage | 40–50 mmHg | 40–50 seconds | 10–12 mmHg |
| Second Stage | 60–80 mmHg | 60–90 seconds | 12–15 mmHg |
9. Formation of forewaters and hind waters- During labour, the bag of membranes containing amniotic fluid is divided by the presenting part of the fetus into two portions:
Forewaters
- The amniotic fluid present in front of the presenting part, between the fetal head and cervix, is called forewaters. During uterine contractions, this fluid forms a tense bag known as the “bag of waters,” which helps in cervical dilatation and protects the fetal head from direct pressure.
Hindwaters
- The amniotic fluid present above and behind the presenting part of the fetus is called hindwaters. It surrounds the fetus inside the uterine cavity and helps maintain intrauterine pressure during labour.
Importance
- Helps in uniform transmission of uterine pressure
- Assists cervical effacement and dilatation
- Protects the fetus and umbilical cord
- Facilitates smooth progress of labour

10. Rupture of the membranes- Rupture of the membranes refers to the breaking of the amniotic sac (bag of waters) with escape of amniotic fluid during labour.
Normally, the membranes rupture spontaneously during the active phase of the first stage of labour when the cervix becomes fully or nearly fully dilated. This is called spontaneous rupture of membranes (SROM).
Types
- Spontaneous rupture of membranes (SROM): Natural rupture during labour
- Artificial rupture of membranes (ARM/Amniotomy): Deliberate rupture by a healthcare provider
- Premature rupture of membranes (PROM): Rupture before onset of labour
- Preterm premature rupture of membranes (PPROM): Rupture before 37 weeks of gestation
Importance
- Helps progress of labour
- Increases effectiveness of uterine contractions
- Allows descent of the presenting part
- Helps assess the colour and amount of amniotic fluid.
11. Show- Show refers to the passage of a small amount of blood-stained mucus from the vagina before or during the onset of labour.
It occurs due to:
- Expulsion of the mucus plug from the cervix
- Rupture of small cervical blood vessels during cervical effacement and dilatation
Importance
- Indicates onset of true labour
- Suggests cervical changes are occurring
12. Fetal axis pressure -Fetal axis pressure is the force transmitted through the long axis of the fetus during uterine contractions. This pressure pushes the presenting part, usually the fetal head, downward against the cervix.
Importance
- Helps cervical effacement and dilatation
- Promotes descent of the fetus
- Assists progress of normal labour
13. Psychological Changes-Excitement, fear, anxiety, and emotional changes occur during labour.These physiological changes help in the normal progress of labour and safe delivery of the baby.
Management Of First Stage of Labour
Principles of Management
- To ensure safety of mother and fetus
- To monitor normal progress of labour
- To detect deviation from normal early
- To maintain asepsis
- To provide comfort and pain relief
- To avoid maternal exhaustion
1. Admission in Labour Room
History Taking
- Onset and duration of pains
- Frequency and duration of contractions
- Passage of show
- Rupture of membranes
- Fetal movements
- Obstetric and medical history
2. General Examination
Observe:
- Pulse-60–100 beats/minute
- Blood pressure-120/80 mmHg(BP ≥140/90 mmHg Hypertension/preeclampsia)
- Temperature-36.5°C–37.5°C
- Respiration-12–20 breaths/minute
- Hydration
- Pallor and edema
3. Abdominal Examination
Assess-
- Height of uterus
- Lie
- Presentation
- Position
- Engagement of head
- Uterine contractions
- Fetal heart sound
Uterine Contractions
Assess-
- Frequency
- Duration
- Intensity
Fetal Heart Rate
Normal-110–160/minute
4. Vaginal Examination
Done under strict aseptic precautions.
Assess-
- Cervical effacement
- Cervical dilatation
- Status of membranes
- Station of presenting part
- Pelvic adequacy
Frequency
- Usually every 4 hours
- Earlier if necessary
5. Preparation of the Woman
- Explain labour process
- Reassure the woman
- Maintain cleanliness
- Provide suitable clothing
- Keep bladder empty
- Encourage companionship and emotional support
6. Monitoring During Labour
A. Maternal Monitoring
- Pulse-Every 30 minutes
- Blood Pressure- Every 4 hours
- Temperature- Every 4 hours
Urine Check for-
- Volume
- Albumin
- Sugar
- Ketones
B. Fetal Monitoring
a. Fetal Heart Sound
- Every 30 minutes in active labour
- After each contraction if high risk
b. Liquor-Observe-
- Colour
- Quantity
- Meconium staining
7. Partograph-Partograph for graphical recording of labour.
It records-
- Cervical dilatation
- Descent of head
- Uterine contractions
- Maternal condition
- Fetal condition
Benefits-
- Detect prolonged labour
- Early identification of obstructed labour
- Timely intervention
8. Diet and Fluids
- Liberal oral fluids allowed
- Light easily digestible diet in early labour
- IV fluids if required
9. Care of Bladder and Bowel
- Encourage urination every 2–3 hours
- Catheterization if bladder is full and woman cannot void
- Routine enema is not recommended.
10. Pain Relief
A. Non-Pharmacological
- Reassurance
- Breathing exercises
- Massage
- Relaxation
- Ambulation
B. Pharmacological
- Analgesics
- Sedatives
- Epidural analgesia
11. Rupture of Membranes
Observe-
- Time of rupture
- Colour of liquor
- Amount
- Fetal heart rate after rupture
- Artificial rupture may be done if indicated.
12. Conduct During First Stage
Avoid
- Frequent vaginal examinations
- Unnecessary interference
- Early bearing down efforts
Maintain
- Asepsis
- Maternal comfort
- Emotional support
- Encourage relaxation technique